![]()
Frontline Learning Research Vol. 12 No. 3 (2024)
20 - 44
ISSN 2295-3159
1University of Augsburg, Germany
2 University of Regensburg, Germany
3University of Turku, Finland
4University of Gothenburg, Sweden
5 Vytautas Magnus University, Lithuania
Article received 14 July 2019 / Article revised 10 August 2024 / Accepted 20 August 2024 / Available online 3 September 2024
Expert performance in a domain is often defined as maximal adaptation to stable task constraints. This definition is useful when analysing the vertical transition when novices become experts. However, many workplaces undergo considerable changes and, thus, task constraints change as well. In this paper a complementary conceptualisation of expertise is offered, one that focuses on expert performance as recurring adaptation to dynamic task constraints. This definition is useful when analysing the horizontal transition when experts adapt to dynamically changing work contexts. Using the documentary method, the aim of the present study was to analyze cases of horizontal transitions based on qualitative biographical interview data from five experts reconstructing different types of adaptation to technological change in their domains that they have experienced. Implications for studying horizontal transitions at dynamic worksites are discussed.
Keywords: Expertise; expert performance; change; work; documentary method.
Many professions undergo recurring transformations as they face rapid and constant change owing to frequent technological innovations that challenge the way experts work in these domains. These challenges also concern what constitutes expert performance in novel environments (Billett et al., 2018; Harteis & Goller, 2014; Palonen et al., 2014; Ward et al., 2019), and how experts adapt their practices to technological shifts in a ‘liquid modernity’ (Baumann, 2007). Notably, Boshuizen and Van de Wiel (2014, p. 71) argue that “[n]ew professions may emerge and the tasks currently undertaken by experts will change requiring learning and gradual or revolutionary adaptations.” If we understand expertise as interdependences between human agency, minds, bodies, and digital technological artifacts (Boshuizen et al. 2020; Gegenfurtner et al., 2023; Gruber & Harteis, 2018; Lehtinen et al., 2014; Säljö, 2019; Szulewski et al., 2019), then existing frameworks for understanding expertise and expert performance in dynamically changing contexts need to be reconsidered.
Such reconsideration is afforded by the notion of horizontal transition of expertise. This notion invites an analysis of expertise in dynamic contexts. The focus on horizontal transition of expertise aims to complement existing research on expertise development in relatively stable and well-structured (Burgoyne et al., 2019; De Groot, 1965; Ericsson, 2018) as well as in relatively fluid and ill-structured domains (Hatano & Oura, 2003; Längler et al., 2017; Lehtinen et al., 2020).
Research points to two complementary cases of expertise development: one that concerns vertical transition and one that concerns horizontal transition of expertise. Figure 1 illustrates these cases. Expert performance in the sense of a vertical transition addresses the development from novice to expert as a result of maximal adaptation to stable task constraints. In contrast, expert performance in the sense of a horizontal transition addresses the development and maintenance of expertise as a result of recurring adaptation to dynamic task constraints.
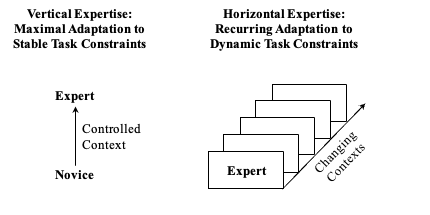
Figure 1. Vertical and horizontal transition of expertise.
Research analysing the vertical transition of a novice becoming an expert often focuses on how experts and novices differ. This line of research is often labelled the contrastive approach, as experts and novices are compared and contrasted with regard to their performance levels and the processes that are hypothesised to lead to different performance levels. These studies often treat the context or task as being relatively stable or predictable. It is no surprise that studies interested in expert performance had their origins in the domain of chess, a highly predictable and well-structured domain with fixed rules and standardised performance measures (De Groot, 1965). Because a highly controlled or ‘representative’ (Ericsson, 2018; Feltovich et al., 2018) task is essential when comparing novices and experts in any given domain, this line of research often collects data in laboratory-like contexts. The analytic focus is descriptive, interested in revealing how and to what extent participants at varying stages of expertise differ.
Studies on horizontal transition are interested in how experts adapt to changing contextual affordances. This line of research tends to differ from research examining vertical transition in several respects. For example, the participant focus is largely on the expert, not because novices are uninteresting, but rather because the main interest is in understanding how experts adapt to contextual change. This line of research is often conducted in and around sociomaterial systems that are characterised by contextual dynamics or ‘moving targets’ (Hoffman et al., 2017). It is no surprise that studies interested in adaptations to change are often conducted in technology-intensive domains (Gruber & Harteis, 2018; Ivarsson et al., 2016; Lehtinen et al., 2014; Lehtinen et al., 2020; Sellberg et al., 2024) because constant introduction of new technologies implies constant adaptations to novel technology-mediated practices (Baumann, 2007; Gegenfurtner et al., 2009; Palonen et al., 2014; Säljö, 2022; Troshani et al., 2018). To capture those developmental trajectories, this line of research often collects data in the field or ‘in the wild’ (Hutchins, 1995). The analytic focus is reconstructive, interested in revealing how experts adapt their practices to novel task affordances (Engeström, 2018).
How does the notion of horizontal transition of expertise relate to other conceptualisations? When describing how experts behave in changing contexts, the literature offers several explanatory frameworks, including the notions of adaptive expertise, knowledge encapsulation, polycontextuality, and expert cognitive flexibility. First, adaptive expertise refers to a highly developed conceptual knowledge base that allows experts to invent novel solutions when environmental constraints change (Anthony et al., 2015; Bohle Carbonell et al., 2014; Lin et al., 2007; Mylopoulos & Woods, 2017). In a classic paper, Hatano and Inagaki (1986) offered the example of a farmer who can effectively deal with contextual covariations such as unusual weather or plant disease. A related example describes an adaptive sushi chef who excels in inventing novel and innovative sushi menus. According to Hatano, adaptive expertise includes three main characteristics: a) the ability to explicate the principles underlying task performance, b) the ability to estimate when routine and non-routine task procedures are necessary, and c) the ability to adapt procedures and solution steps when needed (Hatano & Oura, 2003; Lin et al., 2007). A focus of Hatano’s adaptive expertise approach is on educating students to become adaptive experts, particularly through ‘built-in randomness’ of the teaching material—that is, variability of tasks and contexts to foster transfer of learned knowledge and skills—and a learning climate that encourages active experimentation and play (Hatano & Inagaki, 1986). This approach proves useful not only in undergraduate schooling, but also in professional education, for example when educating forensic specialists (Mustonen & Hakkarainen, 2015), health professionals (Pusic et al., 2018), and teachers (Männikkö & Husu, 2019; Suh et al., 2023). Hatano focuses on the design of learning environments that can foster adaptive expertise in novices; this focus differs from analyses of horizontal transition, which aim at tracing how experts adapt to novel domain affordances.
Second, knowledge encapsulation refers to the clustering of lower-level biomedical knowledge structures into higher-level concepts of greater generality (Boshuizen & Van de Wiel, 2014). Within the realms of encapsulation theory (Boshuizen & Schmidt, 1992), the term describes the cognitive restructuring of knowledge as expertise develops, leading to abbreviations in reasoning processes. These abbreviations explain why experts are faster than novices in task completion (Rikers et al., 2002; Violato & et al., 2018) because experts use encapsulated knowledge concepts. These are further enriched with clinical practice and eventually transformed into illness scripts (Jaarsma, 2015; Strasser & Gruber, 2015). Boshuizen and colleagues argue that, for routine cases inside an expert’s domain, expert biomedical knowledge is encapsulated and integrated into clinical knowledge, while for non-routine cases outside an expert’s domain, biomedical knowledge remains easily accessible when the need arises. Indeed, encapsulation theory has been used to test how experts solve diagnostic problems outside their medical specialty (Rikers et al., 2002), indicating that experts process routine and non-routine clinical case descriptions in qualitatively similar ways. Thus, encapsulation theory is useful to test the robustness of expertise (Boshuizen & Van de Wiel, 2014; Jaarsma, 2015; Violato et al., 2018). While the theory affords a cognitivist analysis of how experts adapt their knowledge-based reasoning processes to dynamic task constraints, to date, encapsulation theory has not been employed to explore how experts adapt their practices when contextual affordances of a domain change.
Third, polycontextuality refers to multiple work tasks, communities of practice, or activity systems within which experts are simultaneously engaged (Engeström, 2018). The concept describes how experts cross the boundaries between parallel activity systems that afford complementary or conflicting participation frameworks. Examples of polycontextual situations include multiprofessional health teams in hospitals or interacting work groups in industrial plants (Engeström, 2018). The focus of polycontextuality is on parallel, already existing activity systems (Dochy et al., 2021). Engeström, Engeström, and Kärkkäinen (1997) convincingly argue that modern work practices are not singular, linear, or stable; instead, “practitioners face the challenge of negotiating and combining ingredients from different contexts to achieve hybrid solutions” as they “operate in and move between multiple, parallel activity systems” (Engeström et al., 1997, p. 442). This observation, made decades ago, has not lost its relevance. Still, while the theoretical notion of polycontextuality is concerned with how experts move between different activity systems, the notion of horizontal transition is on how an activity system changes and how experts adapt to these changes. So the temporal dimension differs between the two notions: polycontextuality is oriented toward presently existing, multiple activity systems and the manoeuvring of experts between them; horizontal transition is oriented toward the development of an activity system from (past to) present to future and how experts accommodate to this development.
Finally, expert cognitive flexibility refers to an expert’s extensive and highly differentiated cognitive schematisation (expert flexibility of type one) and to an expert’s ability to override schema-driven processing to engage in more basic kinds of reasoning (expert flexibility of type two) when confronted with very atypical problems that are infrequent and highly unusual in nature (Spiro et al., 2019) in their domain. For example, medical experts may diagnose rare variations of a medical condition using their knowledge-based flexibility (Feltovich et al., 2018). The essence of cognitive flexibility is in problem solving within one relatively stable domain. Spiro and colleagues (2012) note that when facing a complex new case, “one must assemble just those aspects from prior knowledge that will help in the current situation, while discounting those aspects that are less helpful. Further, the assembled elements must be meaningfully related to each other, and tailored to the specific content of the case at hand to create what Spiro and colleagues call a “schema-of-the-moment” (Spiro et al., 2012, p. 119). Teaching children how to read is a good example here, according to Spiro, because expert teachers will examine each new teaching situation, based on the reading skills of different children, and adapt their teaching strategy flexibly in light of their observations (Spiro et al., 2019). The concept of cognitive flexibility represents a cognitivist perspective with a focus on knowledge and memory; this notion was not designed to reconstruct how experts adapt to changes within their domain. Instead, it is a highly useful framework to analyse how experts deal with problems and challenges within their domain as when teaching children with differing reading skills or when handling rare medical cases.
All these conceptualisations describe how experts flexibly react to and adapt their knowledge and practices to novel or atypical contextual constellations. Adaptive expertise, knowledge encapsulation, and expert cognitive flexibility stress the importance of a highly developed individual knowledge base, while polycontextuality stresses the importance of coordinating elements from different contexts to achieve hybrid solutions. What all these conceptualisations have in common is an interest in atypical or uncertain, yet representative, situations in a domain. In contrast, horizontal transition of expertise occurs when the representativeness of a domain changes. As such, this perspective is useful when analysing how experts adapt their knowledge and practices to changes within existing professional fields—which affords an analytic focus not presently found in expertise theories. More specifically, while Hatano and Inagaki (1986) focus on the design of learning environments that can foster adaptive expertise in novices, this focus differs from analyses of horizontal transitions, which aim at tracing how experts adapt to novel domain affordances. Furthermore, while Boshuizen and Schmidt (1992) afford a cognitivist analysis of how experts adapt their knowledge-based reasoning processes to dynamic task constraints, horizontal transitions of expertise reconstruct how experts adapt their practices when contextual affordances of a domain change. Moreover, while Engeström (2018) is concerned with how experts move between different activity systems, the notion of horizontal transition is on how an activity system changes and how experts adapt to these changes. So the temporal dimension differs between the two notions: polycontextuality is oriented toward presently existing, multiple activity systems and the manoeuvring of experts between them; horizontal transition is oriented toward the development of an activity system from (past to) present to future and how experts accommodate to this development. In addition, Spiro et al. (2012) represent a cognitivist perspective with a focus on knowledge and memory to analyse how experts deal with problems and challenges within their domain while horizontal transitions of expertise put into focus how experts deal with their work when the domain itself changes. In this manuscript, we apply the framework of horizontal transitions of expertise to the domain of medical image diagnosis.
Medical image diagnosis is the interpretation of graphical representations of the human anatomy or its functions (Krupinski, 2018). Examples of medical images are X-ray and computer tomography (CT) scans in radiology; positron emission tomography (PET) images in nuclear medicine; or microscopic images of tissue samples in clinical pathology. Past research has examined how expertise develops in medical image diagnosis (for reviews of this literature, see Gruber et al., 2010; Krupinski, 2018). A large body of studies on expertise in medicine or medical image diagnosis concerns vertical transition of expertise, with typical research questions such as “How do novices develop?” and “How do experts, intermediates, and novices differ?”
Specialised areas of modern medicine increasingly rely on digital technologies. The constant development and implementation of novel digital tools invite an analysis of how established expert practices and routines change. In addressing this topic, a pioneering study by Rystedt and colleagues (2011) examined how experts interpreted an image produced by what was then a new technology, tomosynthesis, and how experts revised their routine practices of seeing. The re-working of their practices aimed at improving diagnostic accuracy and making their diagnoses accountable. Of course, adaptation is not always accomplished easily, and difficulties or problems are frequently encountered (Engeström, 2018; Palonen et al., 2014). The present study deepens and extends first explorations of horizontal transitions published in earlier manuscripts (Gegenfurtner et al., 2009; Lehtinen et al., 2020) and contributes to this line of research by analysing the horizontal transition of expertise induced by technological change in three medical specialties: paediatric radiology, nuclear medicine, and clinical pathology. The rationale for choosing different medical specialties was largely informed by an interest in selecting worksites that are faced with constant invention and implementation of new tools and resources. Adopting a retrospective, biographical perspective in which experts were invited to reflect on their multi-decade working lives, this study pursued the main research question: How and to what extent have experts adapted to technological change in their domains? To elaborate more deeply on these adaptations, we used the documentary method (Bohnsack, 2014; Garfinkel, 1967) as an analytical lens to reconstruct sociogenetic types and to answer a set of associated research questions: Which technological artifacts were introduced in the domain during the course of the experts’ working lives? What was problematic in terms of work practices and ways of knowing after the new artifacts were introduced? What tools or boundary objects did the experts use to adapt their expertise? How did the adaptation evolve? Which factors influenced the adaptation positively or negatively?
To answer the research questions, five experts were interviewed. Four of the experts were the current directors of their units in large university hospitals in Western Finland while the fifth expert was the recently retired director of his unit. One expert was from paediatric radiology, two experts came from clinical pathology, and two experts represented nuclear medicine. All participants were male, had a mean work experience of 27.68 years (± 6.42), and were on average 55.19 years old (± 9.24). The experts were selected based on several criteria, including their age, their experience, their network centrality, their status within the hospital, and their nomination by peers. These are classic criteria used in studies addressing expertise as a vertical development. Since the present study is interested in the participants’ multi-decade professional biographies, this classic set of criteria for addressing vertical transition proved useful also for addressing horizontal transition. Participation in the study was voluntary. Anonymity and confidentiality were guaranteed for all participants.
Retrospective, semi-structured interviews were used to identify horizontal transition of expertise. The interviews aimed at eliciting episodes from the experts’ multi-decade working lives, with a particular focus on how the experts experienced and reported adapting to technological change in their respective domains. Semi-structured qualitative expert interviews are a particularly feasible method here to approach the sociomateriality and hybrid nature of complex expert practices, and how expertise evolves in changing worlds of work (Lehtinen, 2022; Säljö, 2022; Van de Wiel, 2017; Yardley et al., 2019). Van de Wiel (2017, p. 101) state: “As jobs, tasks, equipment, and work roles are not stable but continuously develop, experts in the field par excellence may provide valuable perspectives on future developments, innovations and novel problems and how to deal with them”. The interviews unfolded as a dialogue between the interviewee and the interviewer. All experts were interviewed individually and face-to-face. Interview duration ranged from 50.55 to 90.35 minutes, with an average length of 73.20 minutes (± 11.30) and a total duration of 6 hours and 23.30 minutes. The interviews were recorded and transcribed verbatim. From the interview material, we selected all recorded talk that was associated with technological change and experts’ adaptions to change, with a total duration of 63.30 minutes of interview talk. Other portions of the interviews not selected for analysis included talk about the experts’ families, their education, and their biography and career trajectory. A breakdown of minutes of the selected material per interview is reported in the Appendix.
The interview transcripts were analysed using the documentary method (Bohnsack, 2014; Nohl, 2010). The documentary method is a method for qualitative data analysis that involves searching for patterns underlying a variety of different realisations of meaning. Following Garfinkel (1967, p. 78), utterances in the interview transcripts were treated “as the ‘document of’, as ‘pointing to’, as ‘standing on behalf of’ a presupposed underlying pattern. Not only is the underlying pattern derived from its individual documentary evidences, but the individual documentary evidences, in their turn, are interpreted on the basis of ‘what is known’ about the underlying pattern. Each is used to elaborate the other.” In contrast to other methods for analyzing qualitative interview data, the documentary method aims to reconstruct the interviewees’ own frames of orientation (Bohnsack, 2014) which offers an interpretational framework for understanding, in our study, how the clinical directors adapted to technology changes throughout their professional careers. As Philipps and Mrowczynski (2021, p. 60) observe: “On the one hand, interviewees recapitulate in narrated stories and descriptions how they lived through different biographic events and processes; on the other hand, they often make argumentative or evaluative statements which offer their own interpretations of narrative passages”; the documentary method seeks to reconstruct these frames of orientation experts articulate. In this respect, the documentary method complements other forms of qualitative analyses of expert interviews, such as qualitative content analysis or thematic analysis, which often develop a category scheme, code the interview transcripts based on this scheme, count the occurrence of different codes, and/or visualize interconnections between codes in epistemic network analyses (Gabel et al., in press; Stahnke & Gegenfurtner, in press; Szulewski et al., 2019; Van de Wiel, 2017; White et al., 2018). While such analyses are of course valid, they often seek to contrast experts, intermediates, and novices by adopting the view of vertical transitions. Exploring horizontal transitions, the present study addressed the what and how of expert reconstructions following the documentary method (for more details on the method and step-by-step empirical illustrations, see Beck, 2021; Bohnsack, 2014; Nohl, 2010; Nohl, 2017; Philipps & Mrowczynski, 2021). Particularly, the interview transcripts were analysed in three stages and six steps. Table 1 presents an overview.
Table 1
Stages and Steps in the Documentary Method
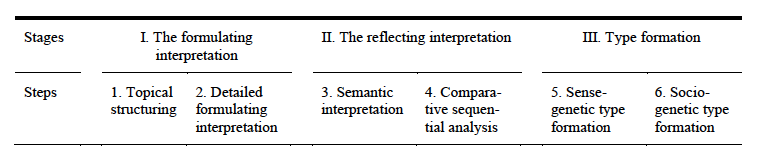
The first stage of the documentary method involved the formulating interpretation. The aim was to establish the “what” of the interview text—that is, the “actual appearance” (Garfinkel, 1967, p. 78) of evidence. Specifically, the interview transcripts were segmented chronologically according to the appearance of topics (step 1: topical structuring). For the purpose of the present study, one topic was chosen for deeper analysis: adaptations to technological change. Transcript segments describing instances of how the experts adapted to technological change were paraphrased and condensed (step 2: detailed formulating structuring).
The second stage of the documentary method involved the reflecting interpretation. The aim was to establish the “how” of the interview text—that is, the “presupposed underlying pattern” (Garfinkel, 1967, p. 78). Specifically, the sequence of topics from stage 1 was semantically interpreted as argumentation, evaluation, description, and narrative (step 3: semantic interpretation). Semantic interpretation was done individually for each interview. For the purpose of the present study, the narratives from step 3 were then compared across the five interviews to analyse the orientation frameworks within which the experts reconstructed their adaptations to technological change (step 4: comparative sequential analysis).
Finally, the last stage of the documentary method involved type formation. The aim was to generate insights into different types of adaptation to technological change in the form of common conclusions across interviews. Specifically, the different orientation frameworks identified in step 4 were abstracted from the interview transcripts and formulated as types in their own right. Specifically, the identified types are given a stand-alone meaning that go beyond the individual interviews; this allows considering maximally contrastive types how experts orient themselves when adapting to technological change (step 5: sense-genetic type formation). The interpretation of these sense-genetic types was finalised using further segments of the interview transcripts to establish and reconstruct the social contexts and constellations within which the experts’ adaptations evolved (step 6: sociogenetic type formation). While the sense-genetic type formation illustrates the different frames of orientations within which the experts react and adapt to domain changes, this sense-genetic type formation cannot illuminate how these different types are embedded in different sociomaterial constellations (Bohnsack, 2014; Nohl, 2017). To unveil these constellations, the sociogenetic type formation draws from additional documentary evidence from other interview parts that illustrate, in our case, what was problematic when new technology was introduced, which tools or boundary objects were used, how adaptations evolved, and which factors influenced the adaptation.
The findings from the documentary method analyses will be presented in three steps. First, we present the outcomes of the formulating interpretation that highlight relevant narratives from the five experts. Second, we report the findings of the interpreting formulation to identify technological change in each medical specialty. Third and finally, we present and describe the resulting type formation that synthesises adaptations to technological change. Figure 2 presents a graphical representation of how the types of adaptation are related to the medical experts’ narratives.
The formulating interpretation analysed the topical structure of each interview. The present study focuses on one of the topics: adaptation to technological change. Results of the detailed formulating interpretation of utterances associated with adaption to technological change are presented for each of the five interviews in the Appendix.
The reflecting interpretation aims at establishing the modus operandi of how the interview narratives describe technological change in the different medical domains. Figure 2 provides an overview. In total, eight instances of significant technological change emerged from the five interviews. The following paragraphs elaborate on these changes and enrich them with text fragments taken from the semantic interpretation of each interview.
3.2.1. From X-ray radiography to computer tomography the semantic interpretation of each interview.
A first change refers to the transition from X-ray radiography to computer tomography in the domain of paediatric radiology. X-ray radiographs are analogous pictures or films that are placed upon a lightbox illuminated from behind to allow viewing the X-ray films with high contrast. In comparison, a computer tomography (CT) digitises the information from the X-ray scanning and presents the pictures on a computer screen with high resolution. Radiographs and computer tomographs use the same underlying processes for creating the pictures. The perceived similarity made an adaptation to this change relatively easy according to the participants. Nowadays, CT is part of the clinical standard in hospitals worldwide. In his narrative describing the transition to digital radiography (Interview 3, 36:25’—36:45’), the expert says: “I have been lucky to see this development quite early. So I got to know this new technology very early. I… I am working in a university hospital. You can learn new tricks every day. That… that… so that makes my life easy, I had that kind of… environment, so I could learn this new trick during my work.”
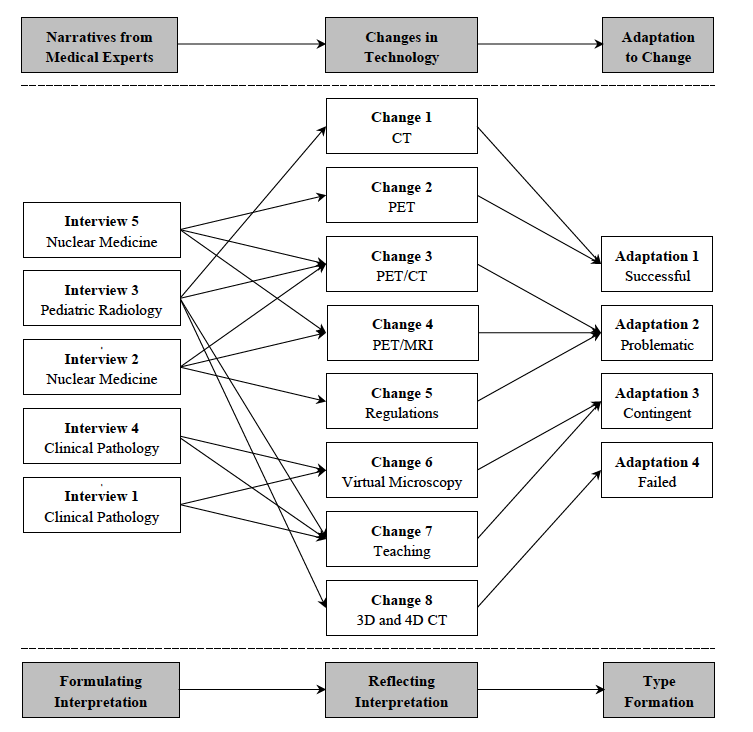
Figure 2. Representation of the data analysis process.
3.2.2. From old versions of PET to new versions of PET
A second change refers to the transition from old versions of positron emission tomography (PET) to newer versions of PET in the domain of nuclear medicine. New hardware and new software were frequently implemented and produced images of increasingly higher resolution. These changes were perceived as making work more convenient. The underlying biophysical processes of image production remained unchanged, so adapting to new versions of PET was relatively easy. As the expert describes it (Interview 5, 22:05’—22:15’): “Of course, in the beginning, you have to become familiar again with the new program… with the new version. But nowadays… the software is so similar. This is all not a big problem.”
3.2.3. From separate images produced by PET and CT to fusion images PET/CT
A third change reported refers to the transition from separate PET and CT images to a novel image type that combines PET and CT into one image, PET/CT. These new fusion images are used in the domains of radiology and nuclear medicine. To interpret PET/CT images correctly, experts need to understand how both elements, PET and CT, are produced. This requires crossing the boundaries from one’s “home” domain to a neighbouring domain as the underlying biophysical processes of image production are radically different. These differences complicate an adaptation, or to use the words of an expert (Interview 5, 29:20’—29:30’): “And this is a problem with it… ok? That the mode and … the style of how different findings are treated is different.” These differences are also evident in the order of the diagnostic practices. Radiologists typically start with interpreting the CT information and continue with interpreting the PET information, while physicians in nuclear medicine “do it just the other way around. I look first at what I can see in the PET and then I look at… where is that what I see in PET… where is that anatomically located and then I look at the surrounding morphology” (narrative from Interview 5, 29:35’—29:50’).
3.2.4. From separate images produced by PET and MR to fusion images PET/MR
Similar to the third change, a fourth change described in the interviews refers to the transition from PET and MR images to a novel image type that combined PET and MRI into one image, PET/MRI. This new fusion technology is used in nuclear medicine. Again, PET/MRI crosses boundaries. To interpret PET/MRI with high diagnostic accuracy, nuclear medicine experts need to leave their “home” domain and learn from another domain. As the expert remembers (Interview 5, 30:10—30:40): “Now this was… much more difficult. Because we have two imaging technologies produced with very, very different underlying principles… That is in the brain… Previously it has been used in neuro… neurosciences. This is exciting. But I had to adapt… really quite… radically different.”
3.2.5. From old regulations to new regulations
A fifth change was associated with the introduction of new regulations, particularly in the domain of nuclear medicine. This change illustrates how governing policies will guide and steer adaptation. Within the context of PET/CT for example, an expert says (Interview 2, 13:15’—13:50’): “When this kind of combination came, it was an immediate question how we can cope with this and … in different countries, this has been solved very differently. I know that… in certain countries, where everything is very tightly regulated… like for example in Germany… then… there is a… all is said by some rules or statutes or whatever… law…that a certain education and training is needed to interpret this case… that is all very strictly regulated, everything that you can do.” These regulations were the basis for implementing training programs. At the same time, new regulations are perceived as increasing cost and slowing down the workflow. These perceptions contribute to a critical attitude toward regulations. “They are… seen artificially to bring more safety but in reality there is very little evidence that the safety is improving… it is just you know the authorities think that the control increases the safety of … or make the life of patients in these studies more safe… but this decision is not based on evidence or rational justification, it is just their gut feelings, and then you know… regulators like to regulate” (35:05—35:20). Adapting to these new regulations and implementing them is described as a frustrating experience. “It’s frustrating in that sense that… as a scientist you would like to see the evidence for these regulations… but this is not the case.” (37:20—37:25).
3.2.6. From light microscopy to virtual microscopy
A sixth change refers to the transition from light microscopy to virtual microscopy in clinical pathology. Virtual microscopy integrates microscopy technology and digital technology and digitises slide sets of tissue samples that can be used for clinical purposes. However, as an expert notes, adaptation from light to virtual microscopy is compromised by image quality of the virtual slides (Interview 1, 39:00’—39:45’): “There are still differences… and especially the… the focusing and the depth of the focusing… it is something that is that is still lacking or is not as far and developed as in the light microscopy… and it’s an important feature… the samples are… the slides are typically 4 or 5 micrometers thick… and the… the… it’s an important diagnostic aid… you can scan the entire sample especially when you are focusing on cellular… cellular details.” And although virtual microscopy is perceived to have high potential for the future of the domain, there was still resistance to change. “If I would have to move to giving diagnoses on the virtual slides, it would be a problem for me, because I am so used to, I have this 25-year history of looking through the microscope” (Interview 1, 57:35’—58:00’). Another expert stated that once he was asking his colleagues what they thought about virtual microscopy or if they use it, the responded that (Interview 4, 21:10’—21:15’). “[t]hey did not like it”. For younger generations, an adaptation might be easier because of their digital nativeness, but for an older generation, change is difficult. “People are lazy animals” (Interview 1, 71:00’—71:05’).
3.2.7. From analogous teaching environments to digital teaching environments
A seventh change refers to the transition from analogous teaching environments to digital teaching environments in the domains of radiology and clinical pathology. Clinical pathology has benefitted from the introduction of virtual microscopy. Although this change has, as we have pointed out, been associated with some problems for clinical work, it is seen as positive for teaching purposes. It eases the availability of study materials and equipment, as one expert argues (Interview 4, 15:35’—15:50’): “When I was young, every student was given a box filled with about 200 slides… this was the traditional way… and now that you have this virtual… virtual microscopy… teaching is basically based on digital images.” The interviews highlight how suitable virtual microscopy is for teaching, and teachers have been using it with considerable success. In radiology, students can access computer tomographic (CT) scans for training purposes at any time from any place. These digital databanks are useful, “but students should… also have access to a teacher when… in case they need one” (Interview 3, 82:40’—82:50’).
3.2.8. From 2D computer tomography to 3D and 4D computer tomography
A final change refers to the transition from two-dimensional to three- and four-dimensional computer tomography images. Two-dimensional CT images resemble analogous X-ray films, while 3D representations allow zooming in and out of the image and use a set of images as if watching a movie. This change from static 2D pictures to 3D pictures was seen as challenging. Even more challenging was the transition to 4D, such as in scans of a pumping heart. Some radiologists face problems in adapting their routines to 3D and 4D. As an expert notes (Interview 3, 39:05’—39:45’): “Some of my colleagues… they look at the 3D data still as if it was 2D… they are going through all the 1000 images… instead of picking up… like… you have to learn new working… practices and a new workflow system… you cannot spend your time looking at all 1000 images carefully but you have to learn a new way how to pick up the information in 3D.” Explanations for the failed adaptation included lack of training and lack of standardised procedures. (Interview 3, 41:45’—41:50’): “There is a generation thing too… especially younger doctors have… are doing it easier.”
Table 2
Sense-Genetic Type Formation
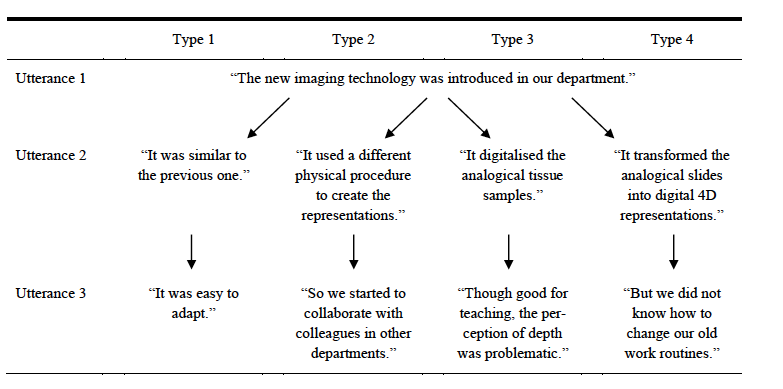
The stage of type formation aimed at abstracting instances of technological change described and clustered in the reflecting interpretation. Type formation included two steps. In a first step, the sense-genetic type formation identified different types of how technological change was reacted to. These instances are interpreted as homologous patterns of adaptation. To illustrate the type formation process, Table 2 presents the four types with utterances from the interview narratives.
In a second step, the four types of adaptations were further contextualised with additional documentary evidence described in the formulating interpretation. This additional documentary evidence helped to reconstruct the social contexts and constellations associated with which the technology introduced; what was problematic after the new technology had been introduced; which tools or boundary objects were used; how the adaptation evolved; and which factors influenced (promoted or hindered) the adaptation process. Ultimately, this analysis resulted in four socio-genetic types of adaptation presented in Table 3: (a) successful adaptation, (b) problematic adaptation, (c) contingent adaptation, and (d) failed adaptation.
3.3.1. Successful adaptation
The type of successful adaptation emerged in narratives related to the transition (a) from X-ray radiography to computer tomography and (b) from old versions to new versions of positron emission tomography. In both cases, the change was associated with lower-level surface changes in image processing, such as an increased resolution and updates of familiar software packages. This perceived surface similarity functioned as a cognitive artifact (in a Vygotskian sense) and successfully mediated the transition from the old technology to the new technology. The interview narratives from both cases illustrate that the adaptation was gradually achieved during regular work practice; it was not accompanied by formal training or regulatory policies. Similarities with the previous technology were perceived as supporting the adaptation.
Table 3
Sociogenetic Types of Adaptation
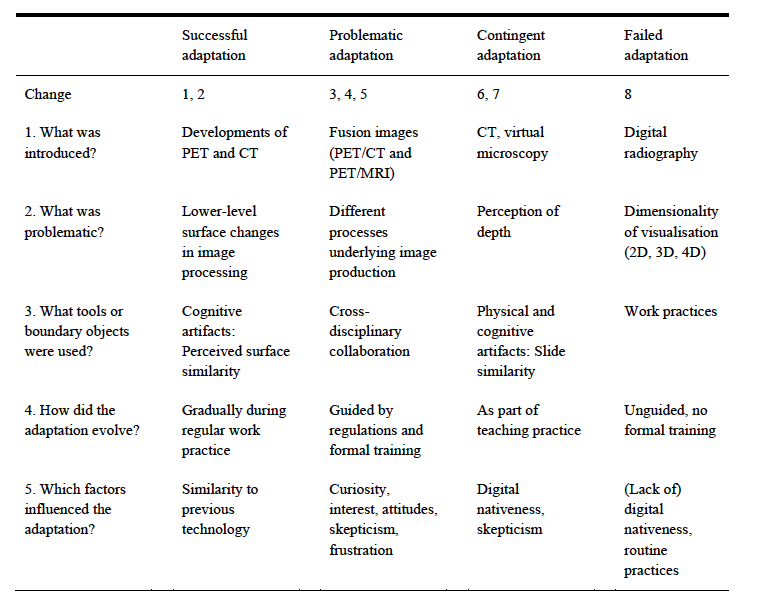
3.3.2. Problematic adaptation
The types of problematic adaptations that emerged in narratives related to the fusion of positron emission tomography with computer tomography (PET/CT) and magnetic resonance imaging (PET/MRI), as well as administrative regulations accompanying these fusion images. What was perceived as being problematic were the different biophysical processes underlying image production, which required cross-disciplinary collaboration with neighbouring specialties. The adaptation process was guided by regulatory bodies that introduced new statutes and control mechanisms, including formal training programs. Factors that promoted the adaptation to technological change were curiosity, interest, and a positive attitude toward digital technologies. Factors that hindered the adaptation process were scepticism with respect to the added value as well as frustration over the regulations introduced. Although the new technologies required great efforts of adaptation, and a level of formal education to cross the boundaries to neighboring disciplines, the adaptation, ultimately, succeeded.
3.3.3. Contingent adaptation
The type of contingent adaptation emerged in narratives related to the transition from (a) light microscopes to virtual microscopy in clinical pathology, and (b) from 2D to 3D computer tomography in radiology. In the case of pathology, the perception of depth was considered problematic for clinical purposes. The similarity between material and digital slides functioned as boundary object that mediated the adaptation process, a process that was hindered by scepticism and lack of digital nativeness that seemed particularly prevalent in older generations of clinical pathologists. Being “sceptic”, which was uttered by the experts, has a connotation of disbelief and unwillingness, while the ground for their hesitations might be more solid. Still, virtual microscopy was successfully introduced and adapted to when the technology was framed as a teaching aid in classrooms. Thus, the adaptation was contingent on the context in which it was used. Virtual microscopy is not replacing light microscopes in clinical work but serves as a resource for medical education and teaching. Similarly, in the case of radiology, a shift from 2D to 3D tomography was successful only when CT scans were used for teaching purposes as a resource for students. Again, while adaptation in the clinical context failed, adaptation in the teaching context succeeded, so success of the adaptation process was contingent on the (teaching) context.
3.3.4. Failed adaptation
The type of failed adaptation emerged in narratives related to the transition from two-dimensional to three- and four-dimensional computer tomography images in clinical radiology contexts. The increased levels of dimensionality were perceived as being very problematic, so routine practices and work flows that had developed around 2D images proved ineffective for 3D and 4D representations of the human anatomy. Adaptation failed because it was unguided by formal training programs or mentored work practices. Additional barriers compromising a horizontal transition of expertise included attitudinal and age-related hindrances associated with not being a ‘digital native’.
The purpose of the present article has been to use the notion of horizontal transition of expertise for the purpose of empirically examining adaptations to technological change reported by medical experts with decades of work experience. Analyses of retrospective, biographical interviews using the documentary method illustrated experiences of a number of technological changes. The way experts reported adapting to these changes differed: While some changes could easily be coped with, other changes were more profound, resulting in problems and even failure in the adaptation process. The analyses also highlight how each horizontal transition of expertise evolved, which tools and boundary objects were used, and which factors promoted or hindered the transition. Promoting factors that were mentioned were formal education and training programs as well as digital nativeness and a positive attitude toward technology. Hindering factors were the lack of training as well as scepticism and the perception that one was too old to adapt. We should also note that, although digital nativeness was mentioned as a promoting factor, younger professionals are not per se digital natives. What is interesting is that technology can sometimes increase image quality (as was the case for radiology and nuclear medicine) and sometimes decrease image quality (as was the case for pathology): the scanning of actual slides for virtual microscopy can result in blurred images that cannot be adapted like in light microscopes; so clinical pathologists miss the advantage of increased image quality the radiologists and nuclear physicians reported. In summary, the interview data helped to reconstruct how and to what extent experts adapted to the turbulences in their working lives produced by the introduction of novel digitised imaging technologies (Boshuizen & Van de Wiel, 2014; Krupinski, 2018; Säljö, 2019).
Conceptually, we offer the notion of horizontal transitions to elaborate on how experts in their domains cope with and adapt to fundamental, disruptive changes and ‘technology shocks’ (rather than minor changes occurring on a more regular basis, assuming that work and life are inherently dynamic). This line of research contributes to the field of expertise research as, to date, a very limited number of studies explore if and how experts adapt when the representativeness of their domain changes. Profound adaptions of these kinds are not easily explained within the framework of routine expertise development as the ‘routine-ness’ of the domain itself transforms as a consequence of contextual changes.
Lehtinen et al. (2020) links expert adaptations to research on conceptual change, particularly to framework theory. Such a perspective is certainly useful because experts can use their rich repertoire of semantic and episodic knowledge stored in working memory—knowledge about clinical concepts, patient cases, medical diagnoses, and the underlying principles of imaging technologies— to better understand changes in their domains than novices can. However, as Lehtinen et al. (2020, p. 4) argue, the described cases “call into question the role of learning new conceptual knowledge and professional practices as well as the kinds of conceptual change processes that are related to initial learning and the subsequent extension of expertise”, which we describe in detail elsewhere (Gegenfurtner et al., 2009; 2017; 2019). There are instances in which experts with a long professional history in one medical arena prefer rigid attempts of using familiar practices to adapt to change, even though these are not effective (cases of failed adaption) while we also see instances of successful adaptions that include the conceptual change of multi-layered professional skills (Lehtinen et al. 2020) constituting the hybridity of expertise (Säljö, 2019; 2022) documented in the multi-decade biographies that were analysed in the present study. Future research may follow Lehtinen et al.’s (2020, p. 8) recommendation to use framework theory “for predicting when the changing of professional practices to adapt to new professional situations is relatively easy and when stronger resistance to change can be expected.”
This study has implications for future research studying expertise and expert performance that should be noted. A first implication relates to a focus on changing contexts. If we conceptualise expertise as being interdependent between human agency, minds, bodies, and digital tools (Billett et al., 2018; Engeström, 2018; Säljö, 2022), and if we further assume that digital tools frequently change in professions (Gekara & Thanh Nguyen, 2018), then we can adopt a relational perspective on expertise, one that is interested in the recurring adaptations of expert work to dynamic task constraints. Such a lens invites an analysis of experts and their professional agency (Billett et al., 2018; Goller & Paloniemi, 2017; Harteis & Goller, 2014) and how experts orient “toward the future, with people not merely repeating past routines but challenging, reconsidering and reformulating their ideas, projects and plans” (Damşa et al., 2017, p. 447). Although it is intuitive to assume that experts need to adapt their practices regularly, there is still a paucity of studies addressing expert performance in changing contexts. This line of research can complement work on expert performance in controlled contexts with representative tasks in well-structured domains that remain relatively unchanged. Such a relational, ontological approach resonates with a lifeworld perspective of expertise in which expertise is conceptualised as “a continuing process of becoming; never entirely complete, nor achieved once and for all” (Dall’Alba, 2018, p. 35). From this perspective, vertical and horizontal expertise development can be analysed as two poles of an analytical continuum.
A second implication for further inquiry relates to replications in fields outside medicine. The medical arena has been selected here because it is a technology-intensive domain with frequent innovations of digital tools and artifacts (Gegenfurtner et al., 2019; Rystedt et al., 2011; Szulewski et al., 2019; Violato et al., 2018; White et al., 2018). But, of course, medicine is not the only domain in which the material affordances of work change. There is good reason to assume that horizontal transition of expertise can be identified in other worksites as well, including, but not limited to, aviation (Hutchins, 1995), architectural design (Degen et al., 2017), accounting (Troshani et al., 2018), teaching (Horlenko et al., 2024; Keskin et al., 2024; Seidel et al., in press), meteorology (Hoffman et al., 2017), or pop music (Längler et al., 2018). It is an interesting question to study if and to what extent the identified sociogenetic types of adaptation to technological change can be found in other high-technology domains or if these adaptation types are intrinsic to medical specialties. For example, the turn to digital teaching in primary, secondary, and higher education institutes worldwide during the Covid 19 pandemic might afford an analysis of the horizontal transitions of teacher expertise. Such work is likely most successful if it follows sociological traditions of expertise research in adopting qualitative analysis (Gobet, 2018; Van de Wiel, 2017; White et al., 2018; Yard et al., 2019).
A third implication for future research relates to conceptual alignments between theories of expertise and theories of transfer. The presented analyses of horizontal transition of expertise touch upon issues associated with transfer of learning. Clearly, the identified instances of horizontal transition can also be read as instances of horizontal transfer in the tradition of ‘innovation’ and ‘multicontextuality’ (Bohle Carbonell et al., 2014; Pusic et al., 2018; Roig et al., 2024; Testers et al., 2015; Testers et al., 2024). If we assume that expertise develops in and across changing contexts (Gruber & Harteis, 2018), then modern workplaces become dynamic sites for invention and reorganisation. As Lehtinen and colleagues (2014, p. 213) state: “How one recognises the familiarity or similarity when entering new situations is important (…). If we shift our focus from very explicit experimental situations of typical transfer studies towards everyday situations or long-term learning of complex scientific or professional tasks, how people interpret the situations and recognise new phenomena with the help of their previously constructed mental concepts is far from trivial.”
A final implication for future work relates to education and training. The analyses indicated that horizontal transition can be unsuccessful, particularly if experts do not receive formal education, training, or mentoring to adapt their practices. Even though the reconstructed narratives seem to suggest that education programs can promote adaptation to technological change, it is of course an empirical question to study how such education programs should be designed, implemented, and monitored to support experts facing technological turbulences in their working lives (Gegenfurtner et al., 2019; Harteis & Goller, 2014; Jossberger et al., 2022; Lehtinen et al., 2020). Addressing these questions is highly important when we seek to understand how experts maintain (Gruber & Harteis, 2018) or renew (Frie et al., 2019) their superior levels of expertise. “The maintenance of expertise is a task which requires a number of people to contribute, both the excellent individual and persons in her or his teams, networks and societies. The expert, with her or his skills and knowledge, continues to work at a high level of performance, even within changing work conditions or societal requirements. The acquired level of expertise, thus, is not an activity at a static level, but the expert has to extend her or his skills and knowledge, which often means to restructure and modify them” (Gruber & Harteis, 2018, p. 110). This restructuring is often facilitated by significant others or persons in the shadow (Längler et al., 2018) that might have potential to function as mediators in managing successful adaptations.
What is frontline when examining cases of horizontal transition of expertise? The argument that we developed and empirically supported in this paper is that the conceptual framework of horizontal transition addresses expertise in changing work contexts in ways no other existing theory does. We do not mean to be disrespectful to the conceptual notions of adaptive expertise, knowledge encapsulation, polycontextuality, or expert cognitive flexibility – quite to the contrary: all these theories have, in our view, very elegantly signified the development of expertise. Still, it is our belief that when we are interested in how experts adapt to changing task requirements in modern workplaces, the notion of horizontal transition proves useful to understand better the corollaries, contingencies, and consequences of these expert adaption processes. Keypoints
Anthony, G., Hunter, J., & Hunter, R. (2015). Prospective
teachers’ development of adaptive expertise. Teaching and
Teacher Education, 49, 108–117.
https://doi.org/10.1016/j.tate.2015.03.010
Baumann, Z. (2007). Liquid times: Living in an age of
uncertainty. Polity Press.
Beck, T. (2021). The praxeological sociology of knowledge–An
introduction to the documentary method and a sketch of an
empirical implementation. In P. J. White, R. Tytler, J. P.
Ferguson, & J. C. Clark (Eds.), Methodological
approaches to STEM education research (Vol. 3, pp.
218–243). Cambridge Scholars Publishing.
Billett, S., Harteis, C., & Gruber, H. (2018). Developing
occupational expertise through everyday work activities and
interactions. In K. A. Ericsson, R. R. Hoffman, A. Kozbelt, &
A. M. Williams (Eds.), Cambridge handbook of expertise and
expert performance (2 nd ed., pp. 105–126).
Cambridge University Press.
https://doi.org/10.1017/9781316480748.008
Bohle Carbonell, K., Stalmeijer, R. E., Könings, K. D., Segers,
M., & Van Merriënboer, J. J. G. (2014). How experts deal with
novel situations: A review of adaptive expertise. Educational
Research Review, 12 , 14–29.
https://doi.org/10.1016/j.edurev.2014.03.001
Bohnsack, R. (2014). Documentary method. In U. Flick (Ed.), Th
e SAGE handbook of qualitative data analysis (pp.
217–233). Sage. https://doi.org/10.4135/9781446282243
Boshuizen, H. P. A., Gruber, H., & Strasser, J. (2020).
Knowledge restructuring through case processing: The key to
generalise expertise development theory across domains? Educational
Research Review, 29, 100310.
https://doi.org/10.1016/j.edurev.2020.100310
Boshuizen, H. P. A., & Schmidt, H. G. (1992). On the role of
biomedical knowledge in clinical reasoning by experts,
intermediates and novices. Cognitive Science, 16(2),
153–184. https://doi.org/10.1016/0364-0213(92)90022-M
Boshuizen, H. P. A., & Van de Wiel, M. W. J. (2014). Expertise
development through schooling and work. In A. Littlejohn & A.
Margaryan (Eds.), Technology-enhanced professional learning:
Processes, practices, and tools (pp. 71–84). Routledge.
Burgoyne, A. P., Nye, C. D., Macnamara, B. N., Charness, N., &
Hambrick, D. Z. (2019). The impact of domain-specific experience
on chess skill: Reanalysis of a key study. American Journal
of Psychology, 132(1), 27–38.
https://doi.org/10.5406/amerjpsyc.132.1.0027
Dall’Alba, G. (2018). Reframing expertise and its development: A
lifeworld perspective. In K. A. Ericsson, R. R. Hoffman, A.
Kozbelt, & A. M. Williams (Eds.), Cambridge handbook of
expertise and expert performance (2 nd ed.,
pp. 33–39). Cambridge University Press.
https://doi.org/10.1017/9781316480748.003
Damşa, C. I., Froehlich, D. E., & Gegenfurtner, A. (2017).
Reflections on empirical and methodological accounts of agency at
work. In M. Goller & S. Paloniemi (Eds.), Agency at
work: An agentic perspective on professional learning and
development (pp. 445–461). Springer.
https://doi.org/10.1007/978-3-319-60943-0_22
Degen, M., Melhuish, C., & Rose, G. (2017). Producing place
atmospheres digitally: Architecture, digital visualisation
practices and the experiences economy. Journal of Consumer
Culture, 17(1), 3–24.
https://doi.org/10.1177/1469540515572238
De Groot, A. D. (1965). Thought and choice in chess.
Mouton.
Engeström, Y. (2018). Expertise in transition: Expansive
learning in medical work . Cambridge University Press.
Engeström, Y., Engeström, R., & Kärkkäinen, M. (1997). The
emerging horizontal dimension of practical intelligence:
Polycontextuality and boundary crossing in complex work
activities. In R. J. Sternberg & E. L. Grigorenko (Eds.), Intelligence,
heredity, and environment (pp. 440–462). Cambridge
University Press.
Ericsson, K. A. (2018). Capturing expert thought with protocol
analysis: Concurrent verbalizations of thinking during experts’
performance on representative tasks. In K. A. Ericsson, R. R.
Hoffman, A. Kozbelt, & A. M. Williams (Eds.), Cambridge
handbook of expertise and expert performance (2 nd
ed., pp. 192–212). Cambridge University Press.
https://doi.org/10.1017/9781316480748.012
Feltovich, P. J., Prietula, M. J., & Ericsson, K. A. (2018).
Studies of expertise from psychological perspectives: Historical
foundations and recurrent themes. In K. A. Ericsson, R. R.
Hoffman, A. Kozbelt, & A. M. Williams (Eds.), Cambridge
handbook of expertise and expert performance (2 nd
ed., pp. 59–83). Cambridge University Press.
https://doi.org/10.1017/9781316480748.006
Frie, L. S., Potting, K. C. J. M., Sjoer, E., Van der Heijden, B.
I. J. M., & Korzilius, H. P. L. M. (2019). How flexperts deal
with changing expertise demands: A qualitative study into the
processes of expertise renewal. Human Resource Development
Quarterly, 30(1), 61–79.
https://doi.org/10.1002/hrdq.21335
Gabel, S., Keskin, Ö., & Gegenfurtner, A. (in press).
Comparing the effects of a specific task instruction and prompts
on pre-service teachers’ noticing of classroom management
situations. Zeitschrift für Erziehungswissenschaft .
Garfinkel, H. (1967). Studies in ethnomethodology.
Prentice Hall.
Gegenfurtner, A., Gruber, H., Holzberger, D., Keskin, Ö.,
Lehtinen, E., Seidel, T., Stürmer, K., & Säljö, R. (2023).
Towards a cognitive theory of visual expertise: Methods of
inquiry. In C. Damşa, A. Rajala, G. Ritella, & J. Brouwer
(Eds.), Re-theorising learning and research methods in
learning research (pp. 146–163). Routledge.
https://doi.org/10.4324/9781003205838-10
Gegenfurtner, A., Lehtinen, E., Helle, L., Nivala, M., Svedström,
E., & Säljö, R. (2019). Learning to see like an expert: On the
practices of professional vision and visual expertise.
International Journal of Educational Research , 98,
280–291. https://doi.org/10.1016/j.ijer.2019.09.003
Gegenfurtner, A., Lehtinen, E., Jarodzka, H., & Säljö, R.
(2017). Effects of eye movement modeling examples on adaptive
expertise in medical image diagnosis. Computers &
Education, 113, 212–225.
https://doi.org/10.1016/j.compedu.2017.06.001
Gegenfurtner, A., Nivala, M., Säljö, R., & Lehtinen, E.
(2009). Capturing individual and institutional change: Exploring
horizontal versus vertical transitions in technology-rich
environments. In U. Cress, V. Dimitrova, & M. Specht (Eds.),
Learning in the synergy of multiple disciplines. Lecture Notes
in Computer Science (pp. 676–681). Springer.
https://doi.org/10.1007/978-3-642-04636-0_67
Gekara, V. O., & Thanh Nguyen, V.-X. (2018). New technologies
and the transformation of work and skills: A study of
computerisation and automation of Australian container terminals.
New Technology, Work and Employment , 33(3),
219–233. https://doi.org/10.1111/ntwe.12118
Gobet, F. (2018). The future of expertise: The need for a
multidisciplinary approach. Journal of Expertise, 1(2),
107–113.
Goller, M., & Paloniemi, S. (Eds.). (2017). Agency at
work: An agentic perspective on professional learning and
development . Springer.
https://doi.org/10.1007/978-3-319-60943-0
Gruber, H., & Harteis, C. (2018). Individual and social
influences on professional learning. Supporting the acquisition
and maintenance of expertise . Springer.
https://doi.org/10.1007/978-3-319-97041-7
Gruber, H., Jansen, P., Marienhagen, J., & Altenmüller, E.
(2010). Adaptations during the acquisition of expertise.
Talent Development & Excellence , 2(1),
3–15.
Harteis, C., & Goller, M. (2014). New skills for new jobs:
Work agency as a necessary condition for successful lifelong
learning. In T. Halttunen, M. Koivisto, & S. Billett (Eds.),
Promoting, assessing, recognizing and certifying lifelong
learning: International perspectives and practices (pp.
37–56). Springer. https://doi.org/10.1007/978-94-017-8694-2_3
Hatano, G., & Inagaki, K. (1986). Two courses of expertise. In
H. Stevenson, H. Asuma, & K. Hakuta (Eds.), Child
development and education in Japan (pp. 262–272).
Freeman.
Hatano, G., & Oura, Y. (2003). Commentary: Reconceptualizing
school learning using insight from expertise research.
Educational Researcher , 32(8), 26–29.
https://doi.org/10.3102/0013189X032008026
Hoffman, R. R., LaDue, D. S., Mogil, M., Roebber, P. J., &
Trafton, J. G. (2017). Minding the weather: How expert
forecasters think. MIT Press.
Horlenko, L., Kaminskienė, L., & Lehtinen, E. (2024). Student
self-regulated learning in teacher professional vision: Results
from combining student self-reports, teacher ratings, and mobile
eye tracking in the high school classroom. Frontline Learning
Research, 12 (2), 51–69.
https://doi.org/10.14786/flr.v12i2.1417
Hutchins, E. (1995). Cognition in the wild. MIT Press.
Ivarsson, J., Rystedt, H., Asplund, S., Johnsson, Å., & Båth,
M. (2016). The application of improved, structured and interactive
group learning methods in diagnostic radiology. Radiation
Protection Dosimetry , 169(1–4), 416–421.
https://doi.org/10.1093/rpd/ncv497
Jaarsma, T. (2015). Expertise development under the
microscope: Visual problem solving in clinical pathology
. Open University of the Netherlands.
Jossberger, H., Breckwoldt, J., & Gruber, H. (2022). Promoting
expertise through simulation (PETS): A conceptual framework.
Learning and Instruction , 82, 1016876.
https://doi.org/10.1016/j.learninstruc.2022.101686
Keskin, Ö., Seidel, T., Stürmer, K., & Gegenfurtner, A.
(2024). Eye-tracking research on teacher professional vision: A
meta-analytic review. Educational Research Review, 42,
100586. https://doi.org/10.1016/j.edurev.2023.100586
Krupinski, E. A. (2018). Perceptual factors in reading medical
images. In E. Samei & E. A. Krupinski (Eds.), Handbook
of medical image perception and techniques (2 nd
ed., pp. 95–106). Cambridge University Press.
https://doi.org/10.1017/9781108163781.008
Längler, M., Nivala, M., & Gruber, H. (2018). Peers, parents
and teachers: A case study on how popular music guitarists
perceive support for expertise development from “persons in the
shadows”. Musicae Scientiae , 22(2),
224–243. https://doi.org/10.1177/1029864916684376
Lehtinen, E. (2022). How to deal with the complexity in research
on workplace learning. In M. Goller, E. Kyndt, S. Paloniemi, &
C. Damşa (Eds.), Methods for researching professional
learning and development (pp. 619–627). Springer.
https://doi.org/10.1007/978-3-031-08518-5_28
Lehtinen, E., Gegenfurtner, A., Helle, L., & Säljö, R. (2020).
Conceptual change in the development of visual expertise.
International Journal of Educational Research , 100,
101545. https://doi.org/10.1016/j.ijer.2020.101545
Lehtinen, E., Hakkarainen, K., & Palonen, T. (2014).
Understanding learning for the professions: How theories of
learning explain coping with rapid change. In S. Billett, C.
Harteis, & H. Gruber (Eds.), International handbook of
research in professional practice-based learning (pp.
199–224). Springer. https://doi.org/10.1007/978-94-017-8902-8_8
Lin, X. D., Schwartz, D. L., & Bransford, J. D. (2007).
Intercultural adaptive expertise: Explicit and implicit lessons
from Dr. Hatano. Human Development , 50(1),
65–72. https://doi.org/10.1159/000097686
Männikkö, I., & Husu, J. (2019). Examining teachers’ adaptive
expertise through personal practical theories. Teaching and
Teacher Education , 77, 126–137.
https://doi.org/10.1016/j.tate.2018.09.016
Mustonen, V., & Hakkarainen, K. (2015). Tracing two
apprentices’ trajectories toward adaptive professional expertise
in fingerprint examination. Vocations and Learning, 8(2),
185–211. https://doi.org/10.1007/s12186-015-9130-7
Mylopoulos, M., & Woods, N. N. (2017). When I say… adaptive
expertise. Medical Education, 51(7), 685–686.
https://doi.org/10.1111/medu.13247
Nohl, A.-M. (2010). The documentary interpretation of narrative
interviews. In R. Bohnsack, N. Pfaff, & W. Weller (Eds.),
Qualitative analysis and documentary method in international
educational research (pp. 195–217). Budrich.
Nohl, A.-M. (2017). Interview und Dokumentarische Methode
[interview and documentary method] (5th ed.). Springer
VS. https://doi.org/10.1007/978-3-658-16080-7
Palonen, T., Boshuizen, H. P. A., & Lehtinen, E. (2014). How
expertise is created in emerging professional fields. In S.
Billett, T. Halttunen, & M. Koivisto (Eds.), Promoting,
assessing, recognizing and certifying lifelong learning:
International perspectives and practices (pp. 131–150).
Springer. https://doi.org/10.1007/978-94-017-8694-2_8
Philipps, A., & Mrowczynski, R. (2021). Getting more out of
interviews. Understanding interviewees’ accounts in relation to
their frames of orientation. Qualitative Research, 21(1),
59–75. https://doi.org/10.1177/1468794119867548
Pusic, M. V., Santen, S. A., Dekhytar, M., Poncelet, A. N.,
Roberts, N. K., Wilson-Delfosse, A. L., & Cutrer, W. B.
(2018). Learning to balance efficiency and innovation for optimal
adaptive expertise. Medical Teacher , 40(8),
820–827. https://doi.org/10.1080/0142159X.2018.1485887
Rikers, R. M. J. P., Schmidt, H. G., Boshuizen, H. P. A., Linssen,
G. C. M., Wesseling, G., & Paas, F. G. W. C. (2002). The
robustness of medical expertise: Clinical case processing by
medical experts and subexperts. American Journal of
Psychology, 115(4), 609–629.
https://doi.org/10.2307/1423529
Roig-Ester, H., Robalino Guerra, P. E., Quesada Pallarès, C.,
& Gegenfurtner, A. (2024). Transfer of learning of new nursing
professionals: Exploring patterns and the effect of previous
working experience. Education Sciences, 14(1),
52. https://doi.org/10.3390/educsci14010052
Rystedt, H., Ivarsson, J., Asplund, S., Johnsson, Å. A., &
Båth, M. (2011). Rediscovering radiology. New technologies and
remedial action at the worksite. Social Studies of Science,
41(6), 867–891. https://doi.org/10.1177/0306312711423433
Säljö, R. (2019). Materiality, learning, and cognitive practices:
Artifacts as instruments of thinking. In T. Cerrato-Pargman &
I. Jahnke (Eds.), Emergent practices and material conditions
in learning and teaching with technologies (pp. 21–32).
Springer. https://doi.org/10.1007/978-3-030-10764-2_2
Säljö, R. (2022). Development, ageing and hybrid minds: Growth and
decline, and ecologies of human functioning in a sociocultural
perspective. Learning, Culture and Social Interaction
, 37, 100465. https://doi.org/10.1016/j.lcsi.2020.100465
Seidel, T., Kosel, C., Böheim, R., Gegenfurtner, A., &
Stürmer, K. (in press). A cognitive model of professional vision
and acquisition of visual expertise using video excerpts in the
teaching profession. In A. Gegenfurtner & R. Stahnke (Eds.),
Teacher professional vision: Theoretical and methodological
advances . Routledge.
Sellberg, C., Nordenström, E., & Säljö, R. (2024). The
development of visual expertise in a virtual environment: A case
of maritime pilots in training. Frontline Learning Research,
12(1), 16–33. https://doi.org/10.14786/flr.v12i1.1217
Spiro, R. J., Feltovich, P. J., Gaunt, A., Hu, Y., Klautke, H.,
Cheng, C., et al. (2019). Cognitive flexibility theory and the
accelerated development of adaptive readiness and adaptive
response to novelty. In P. Ward, J. M. Schraagen, J. Gore, &
E. M. Roth (Eds.), The Oxford handbook of expertise
(pp. 951–976). Oxford University Press.
https://doi.org/10.1093/oxfordhb/9780198795872.013.41
Spiro, R. J., Morsink, P., & Forsyth, B. (2012). Point of
view: Principled pluralism, cognitive flexibility, and new
contexts for reading. In R. F. Flippo (Ed.), Reading
researchers in search of common ground. The expert study
revisited (2 nd ed., pp. 118–128). Routledge.
Stahnke, R., & Gegenfurtner, A. (in press). Beyond analysing
frequencies: Exploring teacher professional vision with epistemic
network analysis of teachers’ think-aloud data. Learning and
Instruction.
Strasser, J., & Gruber, H. (2015). Learning processes in the
professional development of mental health counselors: Knowledge
restructuring and illness script formation. Advances in
Health Sciences Education , 20(2), 515–530.
https://doi.org/10.1007/s10459-014-9545-1
Suh, J. K., Hand, B., Dursun, J. E., Lammert, C., & Fulmer, G.
(2023). Characterizing adaptive teaching expertise: Teacher
profiles based on epistemic orientation and knowledge of epistemic
tools. Science Education , 107(4), 884-911.
https://doi.org/10.1002/sce.21796
Szulewski, A., Braund, H., Egan, R., Gegenfurtner, A., Hall, A.
K., Howes, D., Dagnone, J. D., & Van Merriënboer, J. J. G.
(2019). Starting to think like an expert: An analysis of resident
cognitive processes during simulation-based resuscitation
examinations. Annals of Emergency Medicine , 74(5),
647–659. https://doi.org/10.1016/j.annemergmed.2019.04.002
Szulewski, A., Braund, H., Egan, R., Hall, A. K., Dagnone, J. D.,
Gegenfurtner, A., & Van Merriënboer, J. J. G. (2018). Through
the learner’s lens: Eye-tracking augmented debriefing in medical
simulation. Journal of Graduate Medical Education, 10(3),
340–341. https://doi.org/10.4300/JGME-D-17-00827.1
Testers, L., Alijagic, A., Brand-Gruwel, S., & Gegenfurtner,
A. (2024). Predicting transfer of generic information literacy
competencies by non-traditional students to their study and work
contexts: A longitudinal perspective. Education Sciences,
14(2), 117. https://doi.org/10.3390/educsci14020117
Testers, L., Gegenfurtner, A., & Brand-Gruwel, S. (2015).
Motivation to transfer learning to multiple contexts. In L. Das,
S. Brand-Gruwel, K. Kok, & J. Walhout (Eds.), The school
library rocks: living it, learning it, loving it (pp.
473–487). IASL.
Troshani, I., Janssen, M., Lymer, A., & Parker, L. D. (2018).
Digital transformation of business-to-government reporting: An
institutional work perspective. International Journal of
Accounting Information Systems , 31, 17–36.
https://doi.org/10.1016/j.accinf.2018.09.002
Van de Wiel, M. W. J. (2017). Examining expertise by interviews
and verbal protocols. Frontline Learning Research, 5(3),
94–122. https://doi.org/10.14786/flr.v5i3.257
Violato, C., Gao, H., O’Brien, M. C., Grier, D., & Shen, E.
(2018). How do physicians become medical experts? A test of three
theories: distinct domains, independent influence and encapsulated
models. Advances in Health Sciences Education , 23(2),
249–263. https://doi.org/10.1007/s10459-017-9784-z
Ward, P., Schraagen, J. M., Gore, J., Roth, E. M., Hoffman, R. R.,
& Klein, G. (2019). Reflections on the study of expertise and
its implications for tomorrow’s world. In P. Ward, J. M.
Schraagen, J. Gore, & E. M. Roth (Eds.), The Oxford
handbook of expertise (pp. 1193–1213). Oxford University
Press. https://doi.org/10.1093/oxfordhb/9780198795872.013.52
White, M. R., Braund, H., Howes, D., Egan, R., Gegenfurtner, A.,
Van Merriënboer, J. J. G., & Szulewski, A. (2018). Getting
inside the expert’s head: An analysis of physician cognitive
processes during trauma resuscitations. Annals of Emergency
Medicine, 72(3), 289–298.
https://doi.org/10.1016/j.annemergmed.2018.03.005
Yardley, S., Mattick, K., & Dornan, T. (2019). Close-to-practice
qualitative research. In P. Ward, J. M. Schraagen, J. Gore, &
E. M. Roth (Eds.), The Oxford handbook of expertise
(pp. 408–428). Oxford University Press.
https://doi.org/10.1093/oxfordhb/9780198795872.013.18
The first interview was performed with an expert in clinical
pathology. In the interview, the expert describes the transition
from light microscopes to virtual microscopes (minute 38:25 to
39:55). He then elaborates on how virtual microscopy is used for
teaching (minute 57:35 to 60:40). Finally, the expert describes
age-related differences in the adaptation process (minute 67:05
through 71:30).
38:25’ - 39:55’ Virtual microscopy is introduced in addition to
light microscopes. The perception of depth in virtual slides is
not as good as in electronic microscopes.
57:35’ - 60:40’ Virtual microscopy is used in seminars and
lectures. It is useful and students like it. However, as a teacher
with a 25-year experience in analogical slides, using digital
slides is problematic. Younger teachers familiar with the Interest
and digital media will adapt more quickly because they are digital
natives.
67:05’ - 71:30’ Preference for digital media might be a generation
thing. People are lazy animals. If you have a technique that you
are familiar with and that you like, why not stick to it. A
positive mind for digital media will make adaptation easier.
The second interview was performed with an expert in nuclear
medicine. The expert describes how nuclear medicine has embraced
technological innovations, particularly PET/CT and PET/MRI (minute
6:10 through 18:55). He then describes how the introduction of new
imaging technologies is guided and accompanied by newly
implemented regulations and bureaucratic decisions (minute 28:50
through 37:55).
06:10’ - 18:55’ PET has developed into a fusion technology with
PET/CT and PET/MRI. This requires collaboration with neighbouring
disciplines. Adaptation to PET/CT and PET/MRI is regulated and
organised by law statutes. Training programs are developed to
support the move from PET to PET/CT.
28:50’ - 37:55’ New regulations follow new technologies.
Adaptation to these regulations is necessary, but also frustrating
because the rationale behind regulatory changes does not always
seem evident. Regulators like to regulate.
The third interview was performed with an expert in paediatric
radiology. First, the expert describes the transition from
analogous X-ray radiography to digital computer tomography (CT;
minute 35:50 to 37:05). Second, he elaborates on new developments,
including the introduction of PET/CT and the move from
two-dimensional CT (2D) CT scans to three- (3D) and
four-dimensional (4D) CT scans (minute 37:10 to 38:45). Finally,
he focuses on difficulties associated with adapting to 3D and 4D
CT (minute 38:55 to 46:40).
35:50’ - 37:05’ Traditional X-ray scans are digitised. CT scans
are the new standard. X-ray pictures and 2D CT are very similar.
CT has a higher resolution.
37:10’ - 38:45’ CT is fused with PET into PET/CT images. Training
programs exist for PET/CT reading. 3D and 4D CT scans are
introduced, but no formal training or mentoring programs exist.
38:55’ - 46:40’ Adaptation to 3D and 4D scans is not easy for
everyone. Some colleagues look at 3D and 4D images as they do 2D:
one slide after the other. New practices, a new workflow, are not
yet developed. There is no training. The new generation adapts
more easily because they are digital natives and have developed
this way of digital thinking.
The fourth interview was performed with an expert in clinical
pathology. The expert describes how teaching practices in
classrooms have changed through the introduction of virtual
microscopy (minute 15:25 to 18:35). He then elaborates on
sceptical attitudes toward virtual microscopy for clinical
practice (minute 20:30 to 23:35).
15:25’ - 18:35’ Pathology teaching changed from the use of tissue
samples stored in boxes to the projection of digitised tissue
samples. In lecture halls, virtual microscopy rendered multi-tube
electronic microscopes partially obsolete.
20:30’ - 23:35’ The transition from using light microscopes to
virtual microscopy was slow. In clinical practice, the attitude
toward virtual microscopy was negative because the added value of
virtual microscopy was not immediately clear. Pathological tissue
material can be exchanged globally within a few seconds.
The fifth interview was performed with an expert in nuclear
medicine. The expert first describes developments associated with
positron emission tomography (PET; minute 21:50 to 23:25). In
minutes 23:25 to 24:30 and from 27:00 through 32:25, he describes
very recent innovations including the fusion of PET with computer
tomography (CT) into PET/CT and with magnetic resonance imaging
(MRI) into PET/MRI. Finally, the expert discusses factors that
support or hinder adaptations to technological change (minute
64:50 to 73:55).
21:50’ - 23:25’ The graphical resolution of PET images increased.
Software for analysing the images was updated. New versions of PET
image and software were similar to old versions.
23:25’ - 24:30’ When new imaging technologies are introduced,
formal training is implemented to support staff.
27:00’ - 28:50’ PET is combined with computer tomography (CT).
Radiology and nuclear medicine collaborate. CT images are more
anatomical than PET. Radiology experts start with the CT part,
while nuclear medicine experts start with the PET part. This is a
new challenge for nuclear medicine.
30:10’ - 32:25’ PET is also combined with magnetic resonance
imaging (MRI). Diagnosing with PET/MRI will become much more
difficult because the underlying principles of generating PET and
MR images are very different. The older you become, the more
difficult it is to learn new things. Curiosity is still high, but
also scepticism if technological innovations have any added value.
64:50’ - 73:55’ Interest, curiosity, and scepticism are associated
with novel technologies. If innovations are always rejected, you
risk being outdated and losing patients. Nuclear medicine is a
technological discipline, so people here have a positive attitude
toward technology, a fascination.